심혈관질환(Cardiovascular disease)은 세계적으로 가장 중요한 사망 원인 중하나로, 우리나라의 경우 최근 20년간의 통계를 확인해 볼 때 심혈관질환으로 인한 입원 인구가 2002년부터 2018년 약 4배 정도로 급격하게 증가하고 있는 추세를 보이고 있습니다 1). 이로 인한 경제적 지출 역시 지속적으로 증가할 것으로 생각되며, 이를 조절하기 위해 지난 수십 년간 심혈관질환에 대한 주요 위험 요인(risk factor) 에 대한 연구가 이루어져 왔고, 당뇨나 흡연과 같은 주요 위험요인의 관리 및 적절한 생활습관의 조절과 같은 예방법이 제시되었을 뿐 아니라 저렴한 치료제도 여러 개 개발되었습니다.
그럼에도 불구하고 여전히 심혈관질환의 발생도는 높은 편이며, 이러한 위험 요인들을 좀 더 효율적으로 관리하기 위한 심혈관질환 위험 평가의 필요성이 대두되고 있습니다 2) . 기존에 Framingham Cardiovascular riskassessment, SCORE risk charts, Lipid profile, hsCRP(high-sensitive C-reactive protein) 활용과 같은 여러 종류의 심혈관질환 위험 평가 기법들이 개발되고 사용되어 왔으나 여러 가지 문제점 및 한계를 가지고 있어 추가적인 바이오마커의 필요성이 제기되어 왔습니다 3), 4).
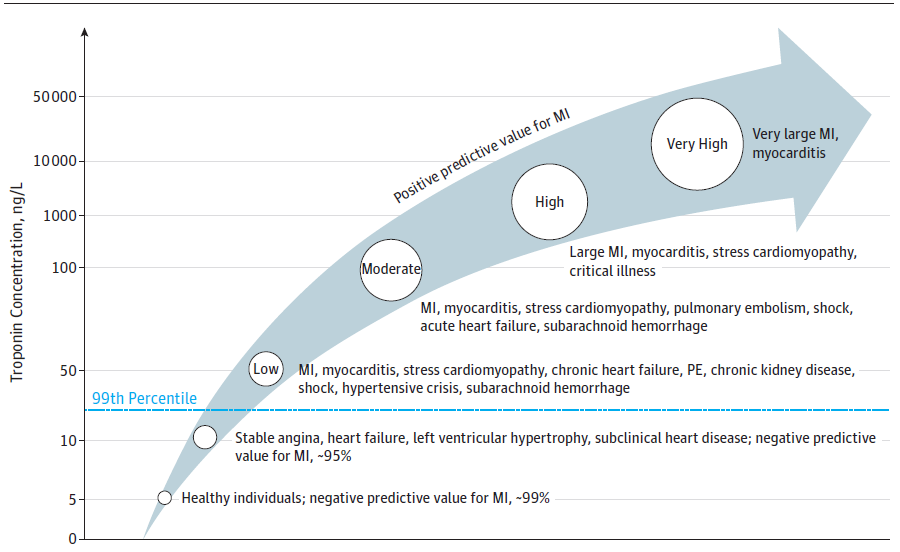 Fig 1 High-sensitive troponin I를 통한 위험도 분류를 통해 파악한 심근손상(Myocardial injury)의 원인4)
Fig 1 High-sensitive troponin I를 통한 위험도 분류를 통해 파악한 심근손상(Myocardial injury)의 원인4)
Cardiac troponin I (cTnI)는 전통적으로 심혈관 질환을 진단하는 일차적인 바이오마커로 임상 현장에서 널리 활용되어 왔으나, 최근 검사법의 발달로 인해 분석민감도가 증가하여 high-sensitive troponin I (hsTnI)검사가 일반화되면서 임상적으로 증상이 나타나지 않지만 추후 심혈관질환으로 인한 사망과 강력하게 연관되어 있는 심근손상 (Myocardial injury)을 확인할 수 있게 되면서 중요한 심혈관질환의 위험도를 사전에 확인할 수 있는 바이오마커로도 주목받고 있습니다4) . 이러한 심근손상은 hsTnI 수치가 99th-percentile 상단을 초과하여 검출되는 경우로 정의되며, 이 경우 환자의 5년 사망률은 약 70%에 달할 뿐 아니라 주요 심혈관질환 이벤트(MACE, major adverse cardiovascular events)를 겪을 확률이 30%에 달하는 것으로 알려져 있습니다 4) .
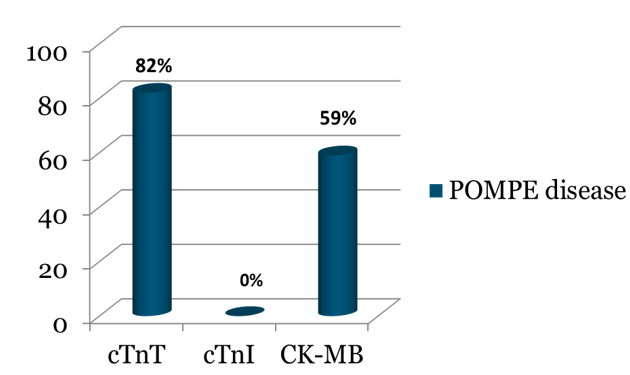 Fig 2 폼페병 환자에서 나타나는 cTnT, cTnI, CK-MB 바이오마커의 증가 5)
Fig 2 폼페병 환자에서 나타나는 cTnT, cTnI, CK-MB 바이오마커의 증가 5)
특히 cTnI의 경우 cardiac troponin T (cTnT), CK-MB와 같은 타 심장 바이오마커에 비해 심근 특이성이 더 좋은 것으로 알려져 있어 심근손상의 위양성 진단률이 더 낮을 것으로 생각될 뿐 아니라5) , cTnT에 비해 상대적으로 더 낮은 diurnal variation을 보이고 있는 등 더 좋은 효율성을 보이고 있으며6) 일반 인구에서의 연구 결과 심근손 상과 더 좋은 연관성을 보여주고 있어 7) 일반 인구를 대상으로 하는 심혈관질환 위험도 평가 가이드 라인에서 구체적인 cut-off 수치가 제시되고 있습니다 8).
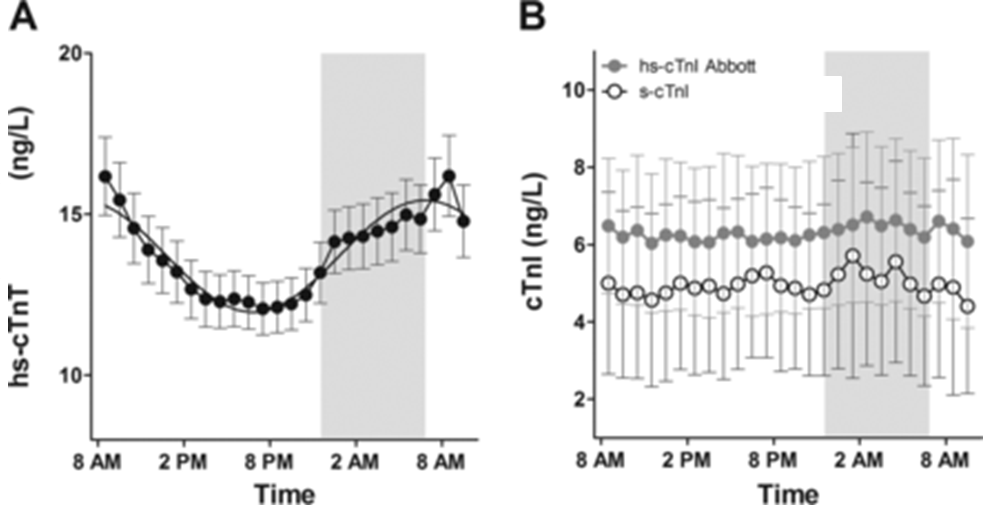 Fig 3 hs-cTnT와 hs-cTnI의 diurnal variation 6)
Fig 3 hs-cTnT와 hs-cTnI의 diurnal variation 6)
Abbott의 high-sensitive Troponin I 검사는 임상 및 진단 결과와 함께 사용할 때 일반 사람들의 미래 심장질환 위험을 더 정확하게 예측하는 데 도움이 되는 최초의 CE 마크 심장 관련 바이오마커이며, 10만명 이상을 대상으로 한 대단위 연구 및 논문을 통한 근거를 갖추고 있는 검사입니다.
Table 1 일반 인구에서의 심근손상 위험도 평가를 위한 cTnI cut-off 8)
| cTnI a | 여성 | 남성 |
|---|---|---|
| Low | < 4 ng/L | <6 ng/L |
| Moderate | 4-10 ng/L | 6-12 ng/L |
| High | >10 ng/L | >10 ng/L |
[REFERENCE]
1) Lee HH, Cho SMJ, Lee H, Baek J, Bae JH, Chung WJ, Kim HC. Korea Heart Disease Fact Sheet 2020: Analysis of Nation-
wide Data. Korean Circ J. 2021. 2 Kim HC. Epidemiology of cardiovascular disease and its risk factors in Korea. Glob Health
Med. 2021 Jun 30;3(3):134-141. doi: 10.35772/ghm.2021.01008. PMID: 34250288; PMCID: PMC8239378.
2) ESC Scientific Document Group, 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed
by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of
Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology
(EAPC), European Heart Journal, Volume 42, Issue 34, 7 September 2021, Pages 3227–3337, https://doi.org/10.1093/
eurheartj/ehab484
3) Lloyd-Jones, Donald M., et al. “Use of risk assessment tools to guide decision-making in the primary prevention of athero-
sclerotic cardiovascular disease: a special report from the American Heart Association and American College of Cardiology.”
Circulation 139.25 (2019): e1162-e1177.
4) McCarthy CP, Raber I, Chapman AR, Sandoval Y, Apple FS, Mills NL, Januzzi JL Jr. Myocardial Injury in the Era of High-Sen-
sitivity Cardiac Troponin Assays: A Practical Approach for Clinicians. JAMA Cardiol. 2019 Oct 1;4(10):1034-1042. doi:
10.1001/jamacardio.2019.2724. PMID: 31389986.
5) Wens, Stephan C A et al. “Elevated Plasma Cardiac Troponin T Levels Caused by Skeletal Muscle Damage in Pompe Dis-
ease.” Circulation. Cardiovascular genetics vol. 9,1 (2016): 6-13. doi:10.1161/CIRCGENETICS.115.001322
6) Klinkenberg LJ, Wildi K, van der Linden N, Kouw IW, Niens M, Twerenbold R, Rubini Gimenez M, Puelacher C, Daniel Neu-
haus J, Hillinger P, Nestelberger T, Boeddinghaus J, Grimm K, Sabti Z, Bons JA, van Suijlen JD, Tan FE, Ten Kate J, Bekers
O, van Loon LJ, van Dieijen-Visser MP, Mueller C, Meex SJ. Diurnal Rhythm of Cardiac Troponin: Consequences for the
Diagnosis of Acute Myocardial Infarction. Clin Chem. 2016 Dec;62(12):1602-1611. doi: 10.1373/clinchem.2016.257485.
Epub 2016 Oct 5. PMID: 27707754.
7) Welsh, Paul, et al. “Cardiac troponin T and troponin I in the general population: comparing and contrasting their genetic de-
terminants and associations with outcomes.” Circulation 139.24 (2019): 2754-2764.
8) Clerico, Aldo, et al. “Evidence on clinical relevance of cardiovascular risk evaluation in the general population using car-
dio-specific biomarkers.” Clinical Chemistry and Laboratory Medicine (CCLM) 59.1 (2021): 79-90.